






Abdurrahman Kadayifci1, Sidart Pradeep2, Eugenia Tsai1,3
1Division of Gastroenterology, UT Health San Antonio, San Antonio, TX, USA; 2Department of Internal Medicine, UT Health San Antonio, San Antonio, TX, USA; 3Department of Hepatology, Texas Liver Institute, San Antonio, TX, USA
Contributions: (I) Conception and design: All authors; (II) Administrative support: E Tsai; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Correspondence to: Eugenia Tsai, MD. Department of Hepatology, Texas Liver Institute, 607 Camden Street, San Antonio, TX 78215, USA; Division of Gastroenterology, UT Health San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78229, USA. Email: tsaie@uthscsa.edu.
Abstract: Acute-on-chronic liver failure (ACLF) represents a rapidly progressive deterioration in chronic liver disease (CLD) marked by multi-organ dysfunction and high short-term mortality. Although consensus on a single definition remains elusive, the clinical phenotype is increasingly recognized across diverse populations, with regional differences in underlying liver disease and precipitants influencing diagnostic criteria and reported incidence. Bacterial infections, alcohol-associated hepatitis (AH), viral hepatitis flares, and drug-induced liver injury (DILI) are among the most common intrahepatic and extrahepatic triggers. The pathophysiology of ACLF reflects immune dysregulation and circulatory collapse, leading to organ failure (OF). This complex interplay may vary according to the number and type of failing organs, the severity of the underlying liver disease, and the nature of the precipitating event. Short-term mortality in ACLF remains high and increases in proportion to the number of OFs. Therapeutic options remain largely supportive, as no disease-modifying therapies have yet been established clinical benefit. Emerging therapies, such as liver support systems, have yet to demonstrate a clear long-term survival advantage. Liver transplantation (LT) remains the sole curative option with demonstrated survival benefit in carefully selected candidates. Due to the high risk of mortality in ACLF, early engagement of palliative care (PC) alongside evaluation for transplant is essential. Early recognition and timely triage remain central to improving outcomes in this high-risk population. This review explores the definitions, prognosis and clinical course of ACLF, emphasizing the importance of early recognition and intervention.
Keywords: Acute-on-chronic liver failure (ACLF); acute decompensation (AD); cirrhosis; organ failure (OF); liver transplantation (LT)
Submitted Aug 05, 2025. Accepted for publication Dec 05, 2025. Published online Jan 15, 2026.
doi: 10.21037/apm-25-84
Introduction
Chronic liver disease (CLD) remains a leading global cause of morbidity and mortality. CLD is the 10th leading cause of death in the USA and 96,110 liver-related deaths were reported in 2023 (1). Due to the significant advances in the prevention and treatment of hepatitis B and C infection, the etiologic landscape of CLD is shifting. Metabolic dysfunction-associated steatotic liver disease [MASLD, formerly non-alcoholic fatty liver disease (NAFLD)] and alcohol-related liver disease (ALD) are rising in parallel with the rising rates of obesity, type 2 diabetes, and alcohol consumption.
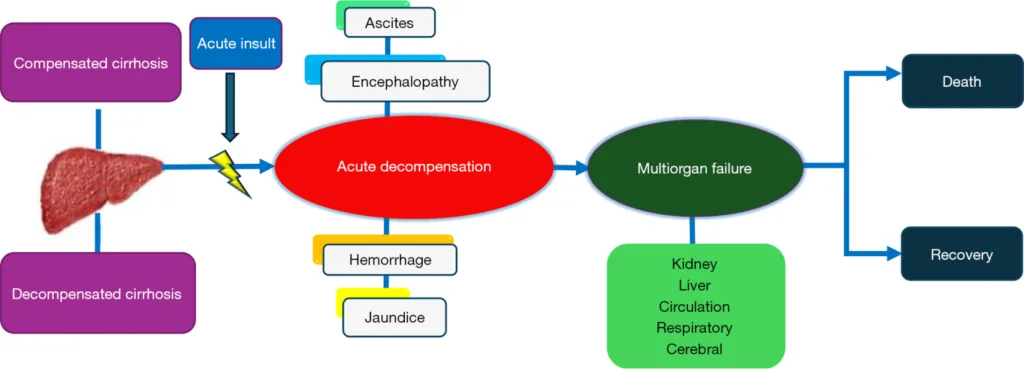
Within this spectrum of chronic injury, acute-on-chronic liver failure (ACLF) has emerged as a syndrome of sudden decompensation and systemic inflammation. Diagnosing ACLF can be challenging due to variability in its definitions across different international consortia. These differing criteria reflect regional differences in etiologies and population characteristics. It is critical to distinguish ACLF from acute decompensation (AD) of cirrhosis, which refers to the acute development of complications of ascites, variceal hemorrhage, hepatic encephalopathy (HE), and jaundice in individuals with cirrhosis, as the clinical course differs significantly. ACLF represents a more severe systemic inflammatory response with multi-organ dysfunction and organ failure (OF). Recognizing this distinction is essential for prognostication and management, as ACLF often requires intensive care and consideration for liver transplantation (LT). Despite its rapid progression and high mortality, ACLF remains potentially reversible with early intervention. Early identification, prevention, and timely treatment of OF are crucial factors that influence survival outcomes. In this clinical review, we aim to explore the current definitions of ACLF, highlight the clinical significance of early identification of ACLF, and summarize key principles of management, with a particular focus on emerging palliative care (PC) strategies.
Defining ACLF
AD in cirrhosis denotes the abrupt onset of major complications such as ascites, HE, gastrointestinal (GI) bleeding, or jaundice—signaling progression from compensated to decompensated disease and a loss of hepatic reserve (2). While AD and ACLF share overlapping triggers, ACLF is characterized by extrahepatic OF and higher short-term mortality (Figure 1). Understanding this distinction is essential for risk stratification, therapeutic planning, and transplant versus palliative decision-making.
The three major international consortia, European Association for the Study of the Liver-Chronic Liver Failure (EASL-CLIF), Asian Pacific Association for the Study of the Liver (APASL) and North American Consortium for the Study of End-Stage Liver Disease (NACSELD) propose differing ACLF definitions reflecting regional differences in etiology and healthcare context (3–5). All agree that ACLF represents acute deterioration in CLD with high 28-day mortality, but differ in the weighting of hepatic versus extrahepatic dysfunction.
EASL-CLIF
In the prospective, multicenter CANONIC study, 1,343 patients with AD of cirrhosis from 29 European centers were evaluated to distinguish ACLF from AD and to establish prognostic grading (4). The EASL-CLIF Consortium derived diagnostic criteria using a modified Sequential Organ Failure Assessment (CLIF-SOFA) score, quantifying dysfunction across six systems—liver, kidney, brain, coagulation, circulation, and respiration (Table 1). ACLF grades 0–3 were assigned according to the number and combination of OFs and demonstrated high 28-day mortality (Table 2).
Table 1
CLIF consortium organ failure score (CLIF-SOFA) (4)
| Variables | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|
| Liver, bilirubin (mg/dL) | 1.2–1.9 | 2.0–5.9 | 6.0–11.9 | ≥12.0 |
| Kidney, creatinine (mg/dL) | 1.2–1.9 | 2.0–3.4 or RRT | 3.5–4.9 or RRT | ≥5.0 or RRT |
| Brain, HE grade (West Haven score) | 1–2 | 3 | 4 | 4 |
| Coagulation, INR | 1.1–1.4 | 1.5–1.9 | 2.0–2.4 | ≥2.5 |
| Circulation, MAP (mmHg) or use of vasopressors | <70 | Dopamine ≤5; dobutamine or terlipressin | Dopamine >5; E or NE ≤0.1 | Dopamine >15; E or NE >0.1 |
| Respiration | ||||
| PaO2/FiO2 | 300–399 | 200–299 | 100–199 | <100 |
| SpO2/FiO2 | 357–511 | 214–356 | 89–213 | <89 |
Table 2
Definition and grading of ACLF by the EASL-CLIF criteria with mortality rates (4)
| ACLF grade | Definition | 28-day mortality (%) | 90-day mortality (%) |
|---|---|---|---|
| 0 | AD of cirrhosis without OF or single non kidney OF and SCr level <1.5 mg/dL and no HE or cerebral failure* and a SCr level <1.5 mg/dL | 4.7 | 14 |
| 1 | Kidney failure; single non kidney OF and SCr 1.5–1.9 mg/dL and/or mild to moderate HE; cerebral failure and SCr 1.5–1.9 mg/dL | 22.1 | 40.7 |
| 2 | 2 OF | 32 | 52.3 |
| 3 | ≥3 OF | 76.7 | 79.1 |
APASL
In 2009, APASL first defined ACLF as an acute hepatic insult leading to jaundice (bilirubin ≥5 mg/dL) and coagulopathy [international normalized ratio (INR) >1.5], complicated by ascites and/or HE within four weeks in patients with CLD (3). Unlike the multiorgan focus of the EASL-CLIF system, the APASL definition centers on hepatic dysfunction as the primary driver of early disease, reflecting etiologic patterns in Asia where HBV reactivation, drug-induced liver injury (DILI), and acute hepatitis E are common precipitants.
The APASL ACLF Research Consortium (AARC) subsequently developed and validated a prognostic score in 1,402 patients with ACLF, identifying bilirubin, creatinine, lactate, INR, and HE grade as independent predictors of 90-day mortality [area under the receiver operating characteristic curve (AUROC) 0.80 derivation; 0.78 validation] (6).
NACSELD
NACSELD defines ACLF as the presence of ≥2 severe extrahepatic OFs in hospitalized patients with cirrhosis, specifically: (I) brain-HE grades III–IV; (II) kidney-renal replacement therapy; (III) respiratory-mechanical ventilation; and (IV) circulatory-vasopressor support. This pragmatic, intensive care unit (ICU)-oriented definition excludes hepatic laboratory criteria, focusing instead on extrahepatic dysfunction and short-term mortality risk. While clinically straightforward, it may underestimate early hepatic-predominant ACLF, thereby omitting patients captured by EASL-CLIF or APASL systems. A United Network for Organ Sharing (UNOS)-based analysis of 48,941 liver transplant candidates showed that 21% met EASL-CLIF criteria, but only 15.3% met NACSELD, highlighting substantial definitional discordance and the broader sensitivity of the EASL-CLIF model. Table 3 summarizes key criteria distinguishing the EASL-CLIF, APASL, and NACSELD frameworks.
Table 3
Characteristics and definitions of ACLF by three major consortia (3–5)
| Characteristics | APASL | EASL-CLIF | NACSELD |
|---|---|---|---|
| Basis of definition | Jaundice and coagulopathy followed by ascites and/or HE within 4 weeks | OF by CLIF-SOFA | ≥2 extrahepatic OF (brain, kidney, respiratory, circulatory) |
| Underlying CLD | Non-cirrhotic CLD compensated cirrhosis | Compensated cirrhosis; decompensated cirrhosis | Decompensated cirrhosis |
| Major acute insults | Alcohol, HBV reactivation, infection | Infection, alcohol, GI bleeding | Bacterial infection |
| Organ failure | Hepatic | Hepatic and/or extrahepatic | Extrahepatic |
| Scoring system | Serum lactate, bilirubin, creatinine, INR and HE | Type and number of OF by EASL-SOFA | Number of extrahepatic OF |
| Mortality rates (7) (28–30 days) | 39% | 48% | 52% |
| Advantages (6,8–10) | Simple assessment | Comprehensive assessment | Simple assessment |
| Early recognition | Captures full spectrum of organ dysfunction | Useful to predict prognosis and mortality | |
| High sensitivity | High sensitivity and risk determination | High specificity and positive predictive value | |
| Applicable to non-cirrhotic patients | |||
| Disadvantages | Low specificity | Complex scoring | Excludes hepatic dysfunction |
| Overlaps with AD | Excludes patients with CLD | Limited early detection | |
| Omits extrahepatic OF | Risk of missing early intervention | Low sensitivity for early grades |
Attempts at unifying ACLF definitions
The absence of a universally accepted definition for ACLF continues to create diagnostic variability across studies and practice settings. The EASL-CLIF framework emphasizes multiorgan failure and short-term mortality; the APASL criteria focus on acute hepatic insult with jaundice and coagulopathy; and the NACSELD definition identifies two or more extrahepatic OFs in hospitalized cirrhotic patients. Recent efforts by the AASLD (2024) and World Gastroenterology Organization (WGO) have sought to harmonize these approaches. Both propose a unified model recognizing ACLF as an acute deterioration of CLD characterized by hepatic failure, one or more extrahepatic OFs, and high short-term mortality (11).
This integrated definition bridges hepatic and extrahepatic perspectives, aiming to improve comparability across regions while supporting earlier recognition of ACLF. In practice, broader AASLD/WGO criteria facilitate timely intervention, whereas the granular grading of EASL-CLIF remains valuable for dynamic prognostication and liver transplant versus PC decision-making.
Etiology and epidemiology of ACLF
The etiology of ACLF can be conceptualized in two distinct stages: (I) underlying CLD and (II) the acute precipitating event. Regional patterns vary significantly between Eastern and Western populations owing to variations in epidemiology, environmental exposure, and healthcare infrastructure. In Eastern countries or regions such as China, Taiwan, and the Philippines, hepatitis B virus (HBV) remains endemic with a 7–9% prevalence, often acquired perinatally, predisposing to HBV reactivation or superinfection due to chronic carrier states (12). In a Chinese cohort of 452 ACLF patients, HBV reactivation accounted for 39.9% of acute insults, with higher 90-day mortality than non-viral causes (36.3% vs. 24.4%, P=0.01) (13).
In Western populations, where HBV prevalence is much lower (~0.3%), ALD, hepatitis C, and MASLD are predominant chronic drivers (14). The EASL-CLIF CANONIC study identified ALD (60.3%), hepatitis C virus (HCV) (13%) or both (9.3%) as the leading etiologies of cirrhosis among ACLF patients, with bacterial infection (32.6%), active alcohol use (24.5%), and GI bleeding (13.2%) as the main precipitants (4). Notably, up to 40–50% of Western cases lack an identifiable trigger, implicating bacterial translocation and systemic inflammation as potential mechanisms (15,16).
Reported ACLF prevalence in patients with CLD varies widely, 7% to 54%, depending on diagnostic criteria and study population (7,17–21). Tertiary-center cohorts report higher rates, up due to referral bias, whereas outpatient studies show lower point prevalence but increasing cumulative incidence—from 14% at 1 year to 41% at 10 years (18,21).
These discrepancies underscore the influence of heterogeneous definitions and populations on reported rates and the challenge of achieving cross-regional epidemiologic comparability.
Pathogenesis of ACLF
Although AD and ACLF share etiologic and precipitating factors, ACLF evolves through a more severe and rapidly progressive course driven by intense systemic inflammation and immune-metabolic dysregulation (11). In advanced cirrhosis, architectural distortion and portal hypertension impair immune surveillance, creating a paradoxical state of immune activation and suppression, termed cirrhosis-associated immune dysfunction (22). This imbalance increases susceptibility to infection, systemic inflammation and multiorgan failure. Increased intestinal permeability and hepatocellular release of pathogen and damage-associated molecular patterns [pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs)], which activate pattern recognition receptors on immune cells, triggering a proinflammatory cascade marked by cytokine release, immune exhaustion, and progressive organ dysfunction (23,24).
A resulting cytokine storm, characterized by elevated levels of interleukin (IL)-6, IL-1, tumor necrosis factor alpha (TNF-α), and IL-8 drives severe systemic inflammation, immune exhaustion, impaired phagocytic function, and ultimately, OF and immune paralysis (25). In the CANONIC study, 15 inflammatory and oxidative markers, including TNF-α, IL-6, IL-8, IL-10, IL-1β, interferon gamma (IFN-γ), IL-17A, monocyte chemoattractant protein-1 (MCP-1), macrophage inflammatory protein-1β (MIP-1β), soluble TNF receptors, and oxidized albumin (HNA2), were quantified across patients with compensated cirrhosis, AD, and ACLF. Elevated baseline levels of IL-6 [odds ratio (OR) 1.43, 95% confidence interval (CI): 1.04–1.96; P=0.03], IL-1ra (OR 1.46, 95% CI: 1.10–1.93; P=0.009), and HNA2 (OR 2.84, 95% CI: 1.52–5.34; P=0.001) independently predicted ACLF development within 28 days (4).
Consistent with the danger hypothesis, DAMPs released from necrotic hepatocytes perpetuate intrahepatic immune activation and cytokine amplification, producing a sepsis-like inflammatory state that accelerates multiorgan failure (26,27). Together, these mechanisms position ACLF as an immunologic tipping point between reversible decompensation and irreversible organ collapse.
Predisposing factors
Baseline risk factors for OF development in ACLF include age, sex, CLD etiology, baseline liver function, and renal function (8). In a prospective cohort, patients with prior decompensations within six months had significantly higher 30-day mortality compared with those patients without (79% vs. 39%, P<0.001) (8). These findings suggest that previous decompensation heightens susceptibility to ACLF progression, underscoring the need for close surveillance and optimization of comorbidities.
Nutritional status also influences outcomes. In a randomized controlled trial (RCT) of dietician-guided outpatient intensive nutrition therapy (OINT) in 70 alcohol-related ACLF, OINT improved 3-month survival (91.4% vs. 57.1%, P<0.001), frailty per the liver frailty index (median delta change of −0.93 vs. −0.33, P<0.00), and disease severity scores, including Model for End-Stage Liver Disease (MELD), MELD-Na and AARC (P<0.05 for all) compared with standard care (28). These results reinforce the importance of targeted nutritional and metabolic optimization as modifiable prognostic factors in ACLF management.
Clinical course and prognosis of ACLF
The clinical course of ACLF is highly dynamic and often unpredictable, evolving over days to weeks. Early identification of patients at risk for progression is crucial for guiding transplant evaluation and level-of-care decisions. In a prospective study observing the clinical course of 388 patients with ACLF during a 28-day period, ACLF worsened in 20.4%, had a steady or fluctuating course in 30.4%, and improved in 49.2% of the cohort (29). Eighty-one percent of patients reached their highest ACLF grade in 3 to 7 days, underscoring that early clinical reassessment is essential to refine prognosis and management. In a retrospective pooled analysis of ACLF patients in the ICU, 90-day mortality among grade 3 EASL-CLIF patients was markedly lower in those who improved by day 3 compared to patients who did not (40%vs. 79%, respectively) (30). These findings highlight that dynamic evaluation within the first week is critical for identifying patients likely to recover with intensive support versus those requiring early transplant consideration or palliative transition. In a 12-week APASL-ACLF study of 453 patients, outcomes based on changes in prothrombin activity and total bilirubin showed 42.4% of patients experienced slow or rapid progression, 9.1% had persistent disease, and 48.5% achieved slow or rapid recovery (31). In a larger APASL cohort of 1,021 patients, recovery from sepsis or OF by day 4 increased transplant eligibility from 37% to 63.7% (32). Conversely, delaying LT up to 7 days was associated with a higher incidence of multiorgan failure, accounting for 23% of deaths within the first week and 55% of all-cause mortality at 28 days. These findings reinforce that early physiologic recovery and timely transplantation are critical determinants of survival in ACLF. The clinical course of ACLF is depicted in Figure 1.
Prognosis
ACLF carries a high short-term mortality that increases with number and severity of OFs, independent of the diagnostic framework used. In the EASL-CLIF CANONIC study, renal failure was the most frequent OF (55.8%), followed by coagulation (27.7%) and cerebral (24.1%) (4). The 28-day mortality rose from 4.7% in patients without OF to 78.6% in those with ≥3 OFs (Table 2) (4). Mortality was also higher in patients without prior AD than those with previous AD (42.2% vs. 29.6%; P=0.03) (4). Patients without ACLF had markedly lower 28- and 90-day mortality, 1.9% and 10%, respectively. In a U.S. Veterans Affairs cohort (n=72,316), 26.4% met ACLF criteria on admission; 28‑ and 90day mortality were 25.5% and 40.0%, respectively (33).
In contrast, the NACSELD cohort identified brain failure (55.7%), circulatory (17.6%) and renal (15.1%) failures as the most common (5). Presence of ≥2 OFs was associated with 30-day mortality of 48% versus 27% for one OF (P<0.0001) (5). External validation using a national dataset showed inpatient survival in ACLF and non-ACLF of 48% and 94%, respectively (P<0.001) (34).
The AARC-ACLF score (range, 5–15) stratifies 28-day mortality into three grades:
- Grade I (5–7 points): 12.7% mortality;
- Grade II (8–10 points): 44.5% mortality;
- Grade III (11–15 points): 85.9% mortality.
Dynamic changes in score during the first week are prognostically informative. Each one-point rise above a score of 10 increased 28-day mortality by ~20% (P=0.001); persistence or progression of grade III over days 4–7 predicted mortality >90% (P<0.001), while downgrade from III to II significantly improved survival (P<0.001) (6). Among 394 patients meeting APASL criteria, those who also satisfied EASL-CLIF criteria had far higher 90-day mortality (59.3% vs. 13.1%, P<0.001), confirming that inclusion of extrahepatic OF enhances risk discrimination (35).
Comparative analyses demonstrate the superior prognostic resolution of EASL-CLIF. In a prospective cohort of 146 hospitalized patients with cirrhosis, EASL-CLIF more accurately predicted 28- and 90-day mortality than either the APASL or NACSELD (AUROC 0.710 and 0.760, respectively; P<0.001) (36). Similarly, a UNOS-based cohort of 48,941 adult liver transplant candidates showed stepwise 30-day mortality across EASL-CLIF grades (from 1.5% in grade 0 to 25.8% in grade 3, P<0.001), whereas NACSELD produced binary separation (28.1% vs. 15.4%) (37). In another prospective study of 468 hospitalized patients, NACSELD achieved higher overall accuracy in predicting 28-day mortality (92.0% vs. 85.3%, P<0.01), with superior specificity (99.7% vs. 84.0%) and positive predictive value (97.1% vs. 50.4%) compared to EASL-CLIF, but at the cost of lower sensitivity (49.3% vs. 92.5%) and negative predictive value (91.6% vs. 98.5%) (38). Thus, EASL-CLIF better captures graded mortality risk and early deterioration, while NACSELD excels in identifying patients at imminent risk of death.
The Chronic Liver Failure Consortium (CLIF-C) AD score was developed for hospitalized cirrhotic patients with AD but without ACLF. Using select parameters, CLIF-C AD score predicted 3- and 12-month mortality better than Child-Pugh, MELD and MELD-Na but use is limited in the ACLF population (39). The CLIF-C ACLF score, developed by the EASL-CLIF Consortium, integrates organ-failure burden, age and leukocyte count to stratify prognosis in patients with ACLF. Validation studies report AUROCs of 0.799±0.078 for 28-day mortality and 0.828±0.063 for 90-day mortality, significantly outperforming MELD, MELD-Na and Child-Turcotte-Pugh (CTP) (P<0.05) (40). In ICU cohorts, a CLIF-C ACLF cutoff ≥70 was associated with >80% 28-day mortality (P=0.006) and marked futility of intensive care support (41).
Together, these scores provide robust tools for stratifying short-term mortality risk in the dynamic changes of ACLF to help guide decision-making around intensive care, transplant eligibility and palliative transitions.
Treatment of ACLF
There is no single curative therapy for ACLF. Management relies entirely on early identification of precipitating factors, prompt organ support and timely risk stratification to prevent progression. Because the syndrome can deteriorate rapidly, early diagnosis and coordinated multidisciplinary care are critical in improving outcomes.
Precipitating factors and associated treatment
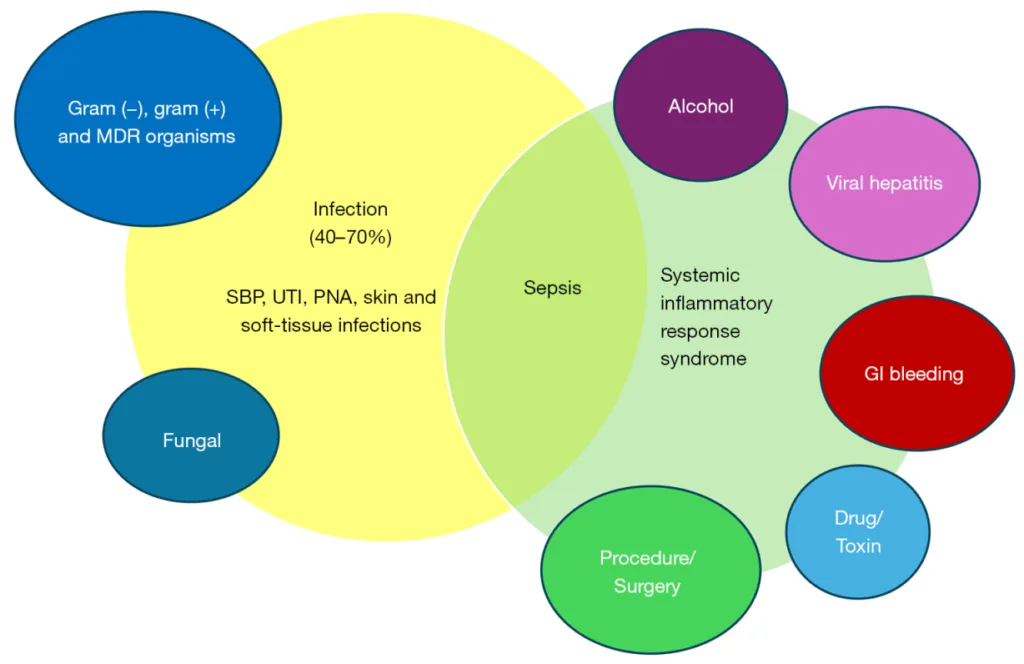
Identification and treatment of precipitating factors are central to ACLF management, with systemic infections accounting for 40–70% of cases (4,9,10). Among these, spontaneous bacterial peritonitis (SBP) is the most frequent, with a prevalence of 20% to 50%, followed by urinary tract infection, pneumonia, and skin or soft tissue infections (9,42). Although gram-negative organisms remain predominant, gram-positive and multi-drug-resistant organisms (MDROs) now constitute up to 32.9% of isolates (5). In a prospective cohort, bacterial infections were identified in 37% of patients at ACLF diagnosis and developed in an additional 46% within four weeks, compared to 25% and 18%, respectively, in patients with AD (P<0.001). Infections, particularly from MDROs, were linked to greater systemic inflammation, progression to ACLF grade 2–3 (47% vs. 26%; P<0.001), and lower 90-day survival (49% vs. 72.5%; P<0.001), with bacterial infection independently predicting mortality in ACLF 1 and ACLF 2 (43). Fungal infections, though less common and accounting <5% but occur predominantly after ACLF onset (78%) and carry a higher 90-day mortality of 71% (43).
In the ICU setting, sepsis is both a precipitant and consequence of ACLF, driving mortality rates of 60–80% among patients with multidrug-resistant (MDR) infections (44). Early recognition and management of sepsis are therefore critical. Key strategies include empiric broad-spectrum coverage guided by local antibiograms and rigorous infection-prevention protocols. Prevention is centered on antimicrobial prophylaxis and early targeted treatment, even in the absence of culture data, given that approximately 50% of such infections are culture-negative (4,43). Each hour of delay increases mortality risk almost two-fold (44). In conjunction with antimicrobial treatment, albumin use reduced the amount of inflammatory mediators such as TNF-alpha (8.2% reduction, P=0.01) from baseline in patients with ACLF and improved overall survival (45).
GI hemorrhage, particularly variceal bleeding, precipitates ACLF through hepatic ischemia, increased gut permeability, and subsequent bacterial translocation (29). Reported prevalence ranges from 13% to 28% (4,46). Management follows established cirrhosis guidelines and includes endoscopic therapy, vasoactive agents, nonselective beta-blockers, and transjugular intrahepatic portosystemic shunt (TIPS) in select patients (47). In those with CTP C cirrhosis (score ≤13), pre-emptive TIPS improves survival with 1-year mortality of 22% compared to 47% in those treated with medical and endoscopic measures (P=0.002) (48). These combined interventions have significantly reduced the mortality associated with variceal hemorrhage.
Invasive procedures, including large volume paracentesis (LVP), TIPS, and surgery precipitate 9% of all cases of ACLF (4,49). Locoregional therapies for hepatocellular carcinoma, including transarterial chemoembolization and radiofrequency ablation, can trigger acute hepatic deterioration in patients with limited hepatic reserve (CTP B or C). In a multicenter retrospective cohort study of 441 ERCPs, ACLF developed in 11.4% of patients with cirrhosis post-procedure and occurred more frequently among those with adverse events (25.9% vs. 8.3%, P=0.01), with MELD score ≥15 and prior decompensation as key risk factors (50). Although data remain limited, procedure appears primarily driven by underlying hepatic dysfunction and procedural complications, emphasizing the need for careful pre-procedure assessment and risk stratification.
Intrahepatic insults constitute a large portion of ACLF precipitants, commonly alcohol-associated hepatitis (AH), acute viral hepatitis, autoimmune hepatitis (AIH) flares, and DILI. AH alone accounts for 24–28% of ACLF cases in Western cohorts (4). Alcohol-related liver injury triggers systemic inflammation and immune dysregulation similar to other causes (4,8). Prevention should focus on sustained abstinence, supported through multi-modal interventions including pharmacotherapy, support programs, and counseling to prevent relapse.
In Asia, acute exacerbation of chronic HBV remains a leading intrahepatic precipitant, responsible for over 50% of ACLF cases in endemic regions (6). Prevention through vaccination, regular monitoring, and timely antiviral treatment remain critical. AIH flares, although less common, frequently precipitate ACLF due to delayed recognition or interruption of immunosuppression. A meta-analysis reported that 12% of patients with AIH flares presenting with ACLF, 71% responded to treatment, but 32% mortality (51). In AIH-related ACLF, glucocorticoid therapy improved 90-day survival when compared with no glucocorticoid therapy (75% vs. 48.1%, P=0.02) (52). DILI, most commonly caused by acetaminophen overdose, herbal supplements, or idiosyncratic reactions to prescribed medications, accounts for 11% of ACLF cases with significantly higher 90-day mortality among drug-induced ACLF as compared with nondrug-induced ACLF (47% vs. 39%; P=0.007) (53). A summary of extra- and intrahepatic precipitants is depicted in Figure 2.
Organ support
Beyond treating precipitating factors, management focuses on supporting failing organ systems to stabilize physiology and improve transplant eligibility.
Kidney
Kidney failure is the most common extrahepatic failure, affecting approximately 55.8% of patients in the CANONIC cohort, and independently associated with 90day mortality [hazard ratio (HR) 1.6–3.3] (3,4,49). Management follows International Club of Ascites (ICA) or Kidney Disease: Improving Global Outcomes (KDIGO) criteria (serum creatinine increase ≥0.3 mg/dL within 48 h or ≥50% within 7 days), and centers on prevention of hepatorenal syndrome (HRS) through nephrotoxin avoidance, early albumin administration (especially in SBP or post-LVP), and circulatory optimization (54). Albumin plus vasoconstrictor therapy is standard, while renal replacement therapy may serve as a bridge to LT.
Circulatory/cardiovascular
Circulatory failure, defined by the need for vasopressor support to maintain mean arterial pressure ≥65 mmHg, reflects severe systemic inflammatory vasodilation. Hemodynamic studies demonstrate a hyperdynamic circulatory state with elevated nitric oxide and tumor necrosis factor levels, reduced vascular resistance, and impaired cardiac response, which further impair organ perfusion and contribute to multiorgan failure (24). Management includes the judicious albumin resuscitation and norepinephrine, with the addition of low-dose vasopressin as an adjunct. In a randomized trial of 100 patients with cirrhosis and sepsis-induced hypotension, 20% albumin achieved faster hemodynamic stabilization than plasmalyte [mean arterial pressure (MAP) >65 mmHg in 62% vs. 22%; P<0.001] and improved lactate clearance, though 28-day mortality was similar (58% vs. 62%, P>0.05) (55). Despite optimized support, circulatory failure portends a poor prognosis, stressing the need for early transplant evaluation.
Respiratory
Respiratory failure may arise from primary pulmonary insults or portal hypertension complications, including hepatic hydrothorax, portopulmonary hypertension, and hepatopulmonary syndrome. Echocardiography aids right heart assessment and guides therapy. In acute respiratory distress syndrome (ARDS), lung-protective ventilation with low tidal volumes (6–8 mL/kg ideal body weight) has been associated with lower mortality (31.0% vs. 39.8%, P=0.007) (56). Although ACLF-specific respiratory management trials are lacking, ventilatory support should be tailored to underlying physiology.
Liver, brain, and coagulation
Progressive hepatic failure manifests as rising total bilirubin and worsening synthetic function, often accompanied by brain and coagulation impairment. HE assessed by the West Haven grade, is a defining feature of all three major definitions of ACLF (3,4,49). HE is a diagnosis of exclusion warranting an evaluation of organic disease, including evaluation of intoxications, substance withdrawal, blood glucose-related disorders, electrolyte disorders, and intracranial pathologies (ischemic or hemorrhagic phenomena), alongside empiric treatment of HE. Lactulose and rifaximin remain the mainstay of treatment. Benefits of polyethylene glycol and ammonia scavengers such as L-ornithine L-aspartate in the acute setting are under study (11,57).
Coagulation status is best assessed with viscoelastic testing with thromboelastography (TEG) and thromboelastometry, which provide real-time functional evaluation of pro- and anticoagulant pathways. A randomized trial of patients with cirrhosis undergoing invasive procedures showed that a TEG-centered strategy led to fewer blood product transfusions relative to a standard INR and platelet count-based strategy (16.7% vs. 100%, P<0.0001) with no difference in bleeding or 90-day mortality (58).
Collectively, these interventions highlight that multisystem stabilization, particularly early renal and circulatory support, remains pivotal in ACLF to serve as both a bridge to recovery and allow for potential LT.
Role of LT
LT remains the only definitive therapeutic intervention for ACLF, and early identification of appropriate candidates is critical to improving survival. In a retrospective cohort study of waitlisted patients with MELD-Na ≥35 and ACLF defined by EASL-CLIF criteria, those with grade 3 ACLF experienced significantly higher 90-day waitlist mortality compared to patients with lower ACLF grades (sub-HR 1.41, 95% CI: 1.12–1.78) (59). These findings suggest that patients with high-grade ACLF may be disadvantaged under the current MELD-based allocation, which does not account for the prognostic impact of extrahepatic OF. Incorporating OF burden into future allocation policies may better reflect transplant urgency in this high-risk population.
PC and hospice
Given the high mortality risk in patients with ACLF grade 2–3, early integration of PC alongside curative-intent management is essential. PC should be introduced ideally at the onset of AD, to optimize symptom management, facilitate goals-of-care discussions, and support decision-making amid potential rapid clinical deterioration. Unfortunately, despite mortality rates exceeding 50% in ACLF grade 2–3, only 30.5% of hospitalized patients with ACLF received PC (32). Utilization remains lowest in older, nonwhite patients with cirrhosis, including those listed for LT (60).
The benefits of early PC involvement are well established. In a large U.S. cohort of alcoholassociated end-stage liver disease, inpatient PC consultation was associated with a significantly reduced 30-day readmission rate (adjusted OR 0.35, 95% CI: 0.31–0.41; P<0.001) and shortened hospitalization duration in those with ACLF score ≥2 (adjusted LOS reduction ~2.34 days; 95% CI: −2.88 to −1.81; P < 0.001) (12). Studies in ESLD show PC consultation lowers procedural burden and hospital costs during terminal admissions (61).
Evidence from transplant and critical care populations confirms that concurrent PC models can be implemented safely without compromising transplant eligibility. Structured PC interventions in the ICU have increased documentation of goals-of-care discussions (2% to 38%), DNR orders (52% to 81%), and reduced length of stay by 3 days without affecting mortality (62).
Transitioning from intensive care to a comfort-centered approach in patients with ACLF should be guided by the reversibility of OF and candidacy for LT. In a prospective multicenter cohort of 2,718 hospitalized patients with cirrhosis, only 5% were discharged to hospice, while 25% of those not discharged to hospice died within six months, highlighting significant underutilization of hospice care (63). Similarly, a qualitative multicenter study involving 42 decompensated cirrhosis found that advance care planning was inconsistently addressed with delays in discussion of prognosis and treatment preferences, leaving patients and surrogates unprepared for end-of-life decisions (64).
Early integration of PC and timely referral to hospice should be pursued in patients to ensure care aligns with patient goals.
Future directions
Management of ACLF relies on prompt treatment of precipitating factors and organ support, while emerging therapies target immunomodulation and extracorporeal support.
In a large phase II trial, granulocyte colony-stimulating factor (G-CSF) failed to improve 90- or 360-day transplant-free survival (HR 1.05; 95% CI: 0.71–1.55; P=0.805) (65). However, a recent meta-analysis (n=603) reported improved 30-, 60-, and 90-day survival with G-CSF [risk ratio (RR) 1.26 (95% CI: 1.10–1.43), 1.47 (95% CI: 1.17–1.84), and 1.73 (95% CI: 1.27–2.35), respectively] (66).
Among liver support systems, both molecular adsorbent recirculating system (MARS) and plasma exchange are emerging therapies. Initial RCTs of MARS in ACLF patients demonstrated improvements in hemodynamics and biochemical parameters, however these early benefits did not translate into a statistically significant survival advantage. In the largest RCT conducted (n=189; 95 treated with MARS vs. 94 standard medical therapy), 28-day mortality did not differ significantly (60.7% vs. 58.9%) (67). Therapeutic plasma exchange has improved short-term, 30-day survival benefit in ACLF (21% vs. 50%, P=0.008) although 90-day mortality was similar (36.8% vs. 52.6%; P=0.166) (68). These findings indicate that while liver support systems may offer temporary benefit, current evidence does not provide clear survival advantage in ACLF.
Predictive analytics has emerged as a new frontier in ACLF management. Advances in artificial intelligence (AI) and machine learning (ML) have produced dynamic, data-driven models that surpass conventional scores such as MELD in predicting short-term mortality and transplant-free survival. The APASL-ACLF Research Consortium Artificial Intelligence (AARC-AI) model, developed from 2,481 patients, achieved an AUROC of 0.91 (validation), outperforming both the day-7 AARC score (+7.0%, P<0.001) and MELD (+12.8%, P<0.001) for 30-day mortality prediction (69). These AI-based tools offer dynamic, individualized prognostication and may enhance early triage and clinical decision-making in ACLF.
Conclusions
ACLF is a distinct clinical entity characterized by AD of CLD, rapid progression to OF, and substantial short-term mortality. Early recognition is critical, as treatment remains largely supportive and outcomes hinge on timely identification of precipitants and risk stratification. While a subset of patients may be candidates for LT, many experience clinical decline, emphasizing the need for early integration of PC to align treatment goals, manage symptoms, and guide decision-making in the face of this rapidly evolving and life-threatening syndrome.
Footnote
Peer Review File: Available at https://apm.amegroups.com/article/view/10.21037/apm-25-84/prf
Funding: None.
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://apm.amegroups.com/article/view/10.21037/apm-25-84/coif). The authors have no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Open Access Statement: This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
References
- Ahmad FB, Cisewski JA, Anderson RN. Leading Causes of Death in the US, 2019-2023. JAMA 2024;332:957-8. [Crossref] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol 2018;69:406-60. Erratum in: J Hepatol 2018;69:1207. [Crossref] [PubMed]
- Sarin SK, Kumar A, Almeida JA, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the study of the liver (APASL). Hepatol Int 2009;3:269-82. [Crossref] [PubMed]
- Moreau R, Jalan R, Gines P, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013;144:1426-37, 1437.e1-9.
- Bajaj JS, O’Leary JG, Reddy KR, et al. Survival in infection-related acute-on-chronic liver failure is defined by extrahepatic organ failures. Hepatology 2014;60:250-6. [Crossref] [PubMed]
- Choudhury A, Jindal A, Maiwall R, et al. Liver failure determines the outcome in patients of acute-on-chronic liver failure (ACLF): comparison of APASL ACLF research consortium (AARC) and CLIF-SOFA models. Hepatol Int 2017;11:461-71. [Crossref] [PubMed]
- Mahmud N, Kaplan DE, Taddei TH, et al. Incidence and Mortality of Acute-on-Chronic Liver Failure Using Two Definitions in Patients with Compensated Cirrhosis. Hepatology 2019;69:2150-63. [Crossref] [PubMed]
- Jalan R, Stadlbauer V, Sen S, et al. Role of predisposition, injury, response and organ failure in the prognosis of patients with acute-on-chronic liver failure: a prospective cohort study. Crit Care 2012;16:R227. [Crossref] [PubMed]
- Wong F, Piano S, Singh V, et al. Clinical features and evolution of bacterial infection-related acute-on-chronic liver failure. J Hepatol 2021;74:330-9. [Crossref] [PubMed]
- Medhat MA, Gushken F, Khaled T, et al. Acute-on-chronic liver failure in Egypt: an underestimated complication of liver cirrhosis. Eur J Gastroenterol Hepatol 2021;33:e458-63. [Crossref] [PubMed]
- Karvellas CJ, Bajaj JS, Kamath PS, et al. AASLD Practice Guidance on Acute-on-chronic liver failure and the management of critically ill patients with cirrhosis. Hepatology 2024;79:1463-502. [Crossref] [PubMed]
- GBD 2019 Hepatitis B Collaborators. Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol 2022;7:796-829. [Crossref] [PubMed]
- Liang J, Liu L, Cao Y, et al. Hepatitis B-related acute-on-chronic liver failure induced by hepatotropic viral insult is associated with worse prognosis than that induced by non-virus insult. BMC Infect Dis 2021;21:1273. [Crossref] [PubMed]
- Hyun Kim B, Ray Kim W. Epidemiology of Hepatitis B Virus Infection in the United States. Clin Liver Dis (Hoboken) 2018;12:1-4. [Crossref] [PubMed]
- Thanapirom K, Suksawatamnuay S, Wejnaruemarn S, et al. Bacterial DNA Translocation Is Associated With Overt Hepatic Encephalopathy and Mortality in Patients With Cirrhosis. Clin Transl Gastroenterol 2024;15:e00697. [Crossref] [PubMed]
- Kou K, Sun X, Tian G, et al. The Mechanisms of Systemic Inflammatory and Immunosuppressive Acute-on-Chronic Liver Failure and Application Prospect of Single-Cell Sequencing. J Immunol Res 2022;2022:5091275. [Crossref] [PubMed]
- Aggarwal A, Biswas S, Arora U, et al. Definitions, Etiologies, and Outcomes of Acute on Chronic Liver Failure: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol 2024;22:2199-2210.e25. [Crossref] [PubMed]
- Chirapongsathorn S, Teerasarntipan T, Tipchaichatta K, et al. Acute-on-chronic liver failure: Epidemiology, prognosis, and outcome of a multicenter study in Thai population. JGH Open 2022;6:205-12. [Crossref] [PubMed]
- Qin G, Shao JG, Zhu YC, et al. Population-representative Incidence of Acute-On-Chronic Liver Failure: A Prospective Cross-Sectional Study. J Clin Gastroenterol 2016;50:670-5. [Crossref] [PubMed]
- Mezzano G, Juanola A, Cardenas A, et al. Global burden of disease: acute-on-chronic liver failure, a systematic review and meta-analysis. Gut 2022;71:148-55. [Crossref] [PubMed]
- Piano S, Tonon M, Vettore E, et al. Incidence, predictors and outcomes of acute-on-chronic liver failure in outpatients with cirrhosis. J Hepatol 2017;67:1177-84. [Crossref] [PubMed]
- Albillos A, Lario M, Álvarez-Mon M. Cirrhosis-associated immune dysfunction: distinctive features and clinical relevance. J Hepatol 2014;61:1385-96. [Crossref] [PubMed]
- Qiang R, Liu XZ, Xu JC. The Immune Pathogenesis of Acute-On-Chronic Liver Failure and the Danger Hypothesis. Front Immunol 2022;13:935160. [Crossref] [PubMed]
- Casulleras M, Zhang IW, López-Vicario C, et al. Leukocytes, Systemic Inflammation and Immunopathology in Acute-on-Chronic Liver Failure. Cells 2020;9:2632. [Crossref] [PubMed]
- Cao M, Wang G, Xie J. Immune dysregulation in sepsis: experiences, lessons and perspectives. Cell Death Discov 2023;9:465. [Crossref] [PubMed]
- Wiest R, Lawson M, Geuking M. Pathological bacterial translocation in liver cirrhosis. J Hepatol 2014;60:197-209. [Crossref] [PubMed]
- Antoniades CG, Quaglia A, Taams LS, et al. Source and characterization of hepatic macrophages in acetaminophen-induced acute liver failure in humans. Hepatology 2012;56:735-46. [Crossref] [PubMed]
- Giri P, Taneja S, Sahni N, et al. Outpatient Intensive Nutrition Therapy Improves Survival and Frailty in Males With Alcohol-related ACLF – Randomized Controlled Trial. Clin Gastroenterol Hepatol 2025;23:1164-1173.e2. [Crossref] [PubMed]
- Gustot T, Fernandez J, Garcia E, et al. Clinical Course of acute-on-chronic liver failure syndrome and effects on prognosis. Hepatology 2015;62:243-52. [Crossref] [PubMed]
- Karvellas CJ, Garcia-Lopez E, Fernandez J, et al. Dynamic Prognostication in Critically Ill Cirrhotic Patients With Multiorgan Failure in ICUs in Europe and North America: A Multicenter Analysis. Crit Care Med 2018;46:1783-91. [Crossref] [PubMed]
- Xu MM, Kong M, Yu PF, et al. Clinical Course and Outcome Patterns of Acute-on-chronic Liver Failure: A Multicenter Retrospective Cohort Study. J Clin Transl Hepatol 2021;9:626-34. [Crossref] [PubMed]
- Choudhury A, Vijayaraghavan R, Maiwall R, et al. ‘First week’ is the crucial period for deciding living donor liver transplantation in patients with acute-on-chronic liver failure. Hepatol Int 2021;15:1376-88. [Crossref] [PubMed]
- Hernaez R, Kramer JR, Liu Y, et al. Prevalence and short-term mortality of acute-on-chronic liver failure: A national cohort study from the USA. J Hepatol 2019;70:639-47. [Crossref] [PubMed]
- Rosenblatt R, Shen N, Tafesh Z, et al. The North American Consortium for the Study of End-Stage Liver Disease-Acute-on-Chronic Liver Failure Score Accurately Predicts Survival: An External Validation Using a National Cohort. Liver Transpl 2020;26:187-95. [Crossref] [PubMed]
- Zhang Q, Li Y, Han T, et al. Comparison of current diagnostic criteria for acute-on-chronic liver failure. PLoS One 2015;10:e0122158. [Crossref] [PubMed]
- Leão GS, Lunardi FL, Picon RV, et al. Acute-on-chronic liver failure: A comparison of three different diagnostic criteria. Ann Hepatol 2019;18:373-8. [Crossref] [PubMed]
- Lee BP, Cullaro G, Vosooghi A, et al. Discordance in categorization of acute-on-chronic liver failure in the United Network for Organ Sharing database. J Hepatol 2022;76:1122-6. [Crossref] [PubMed]
- Cao Z, Liu Y, Cai M, et al. The Use of NACSELD and EASL-CLIF Classification Systems of ACLF in the Prediction of Prognosis in Hospitalized Patients With Cirrhosis. Am J Gastroenterol 2020;115:2026-35. [Crossref] [PubMed]
- Jalan R, Pavesi M, Saliba F, et al. The CLIF Consortium Acute Decompensation score (CLIF-C ADs) for prognosis of hospitalised cirrhotic patients without acute-on-chronic liver failure. J Hepatol 2015;62:831-40. [Crossref] [PubMed]
- Barosa R, Roque Ramos L, Patita M, et al. CLIF-C ACLF score is a better mortality predictor than MELD, MELD-Na and CTP in patients with Acute on chronic liver failure admitted to the ward. Rev Esp Enferm Dig 2017;109:399-405. [Crossref] [PubMed]
- Engelmann C, Thomsen KL, Zakeri N, et al. Validation of CLIF-C ACLF score to define a threshold for futility of intensive care support for patients with acute-on-chronic liver failure. Crit Care 2018;22:254. [Crossref] [PubMed]
- Liu XQ, Zhang XY, Ying Y, et al. The role of prophylactic antibiotics in hepatitis B virus-related acute-on-chronic liver failure patients at risk of bacterial infection: a retrospective study. Infect Dis Poverty 2021;10:44. [Crossref] [PubMed]
- Fernández J, Acevedo J, Wiest R, et al. Bacterial and fungal infections in acute-on-chronic liver failure: prevalence, characteristics and impact on prognosis. Gut 2018;67:1870-80. [Crossref] [PubMed]
- Ndomba N, Soldera J. Management of sepsis in a cirrhotic patient admitted to the intensive care unit: A systematic literature review. World J Hepatol 2023;15:850-66. [Crossref] [PubMed]
- Fernández J, Clària J, Amorós A, et al. Effects of Albumin Treatment on Systemic and Portal Hemodynamics and Systemic Inflammation in Patients With Decompensated Cirrhosis. Gastroenterology 2019;157:149-62. [Crossref] [PubMed]
- Zhao H, Zhao R, Hu J, et al. Upper gastrointestinal hemorrhage in acute-on-chronic liver failure: prevalence, characteristics, and impact on prognosis. Expert Rev Gastroenterol Hepatol 2019;13:263-9. [Crossref] [PubMed]
- Garcia-Tsao G, Abraldes JG, Berzigotti A, et al. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017;65:310-35. [Crossref] [PubMed]
- Hernández-Gea V, Procopet B, Giráldez Á, et al. Preemptive-TIPS Improves Outcome in High-Risk Variceal Bleeding: An Observational Study. Hepatology 2019;69:282-93. [Crossref] [PubMed]
- O’Leary JG, Reddy KR, Garcia-Tsao G, et al. NACSELD acute-on-chronic liver failure (NACSELD-ACLF) score predicts 30-day survival in hospitalized patients with cirrhosis. Hepatology 2018;67:2367-74. [Crossref] [PubMed]
- Leal C, Prado V, Colan J, et al. Adverse Events and Acute Chronic Liver Failure in Patients With Cirrhosis Undergoing Endoscopic Retrograde Cholangiopancreatography: A Multicenter Matched-Cohort Study. Am J Gastroenterol 2019;114:89-97. [Crossref] [PubMed]
- Patil AN, Shamim MA, Roy A, et al. Prevalence of Acute on Chronic Liver Failure in Autoimmune Hepatitis, Treatment Response and Mortality Burden Assessment: A Region-Predominant Systematic Review and Meta-Analysis. J Clin Gastroenterol 2024;58:564-9. [Crossref] [PubMed]
- Anand L, Choudhury A, Bihari C, et al. Flare of Autoimmune Hepatitis Causing Acute on Chronic Liver Failure: Diagnosis and Response to Corticosteroid Therapy. Hepatology 2019;70:587-96. [Crossref] [PubMed]
- Devarbhavi H, Choudhury AK, Sharma MK, et al. Drug-Induced Acute-on-Chronic Liver Failure in Asian Patients. Am J Gastroenterol 2019;114:929-37. [Crossref] [PubMed]
- Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract 2012;120:c179-84. [Crossref] [PubMed]
- Maiwall R, Kumar A, Pasupuleti SSR, et al. A randomized-controlled trial comparing 20% albumin to plasmalyte in patients with cirrhosis and sepsis-induced hypotension J Hepatol 2022;77:670-82. [ALPS trial]. [Crossref] [PubMed]
- Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000;342:1301-8. [Crossref] [PubMed]
- Sidhu SS, Sharma BC, Goyal O, et al. L-ornithine L-aspartate in bouts of overt hepatic encephalopathy. Hepatology 2018;67:700-10. [Crossref] [PubMed]
- De Pietri L, Bianchini M, Montalti R, et al. Thrombelastography-guided blood product use before invasive procedures in cirrhosis with severe coagulopathy: A randomized, controlled trial. Hepatology 2016;63:566-73. [Crossref] [PubMed]
- Sundaram V, Shah P, Mahmud N, et al. Patients with severe acute-on-chronic liver failure are disadvantaged by model for end-stage liver disease-based organ allocation policy. Aliment Pharmacol Ther 2020;52:1204-13. [Crossref] [PubMed]
- Oliveira HM, Miranda HP, Rego F, et al. Palliative care and end stage liver disease: A cohort analysis of palliative care use and factors associated with referral. Ann Hepatol 2024;29:101518. [Crossref] [PubMed]
- Patel AA, Walling AM, Ricks-Oddie J, et al. Palliative Care and Health Care Utilization for Patients With End-Stage Liver Disease at the End of Life. Clin Gastroenterol Hepatol 2017;15:1612-1619.e4. [Crossref] [PubMed]
- Lamba S, Murphy P, McVicker S, et al. Changing end-of-life care practice for liver transplant service patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage 2012;44:508-19. [Crossref] [PubMed]
- O’Leary JG, Tandon P, Reddy KR, et al. Underutilization of Hospice in Inpatients with Cirrhosis: The NACSELD Experience. Dig Dis Sci 2020;65:2571-9. [Crossref] [PubMed]
- Patel AA, Ryan GW, Tisnado D, et al. Deficits in Advance Care Planning for Patients With Decompensated Cirrhosis at Liver Transplant Centers. JAMA Intern Med 2021;181:652-60. [Crossref] [PubMed]
- Engelmann C, Herber A, Franke A, et al. Granulocyte-colony stimulating factor (G-CSF) to treat acute-on-chronic liver failure: A multicenter randomized trial (GRAFT study). J Hepatol 2021;75:1346-54. [Crossref] [PubMed]
- Qiu B, Liang JX, Romero Gómez M. The efficacy and safety of granulocyte colony-stimulating factor in the treatment of acute-on-chronic liver failure: A systematic review and meta-analysis. PLoS One 2023;18:e0294818. [Crossref] [PubMed]
- Bañares R, Nevens F, Larsen FS, et al. Extracorporeal albumin dialysis with the molecular adsorbent recirculating system in acute-on-chronic liver failure: the RELIEF trial. Hepatology 2013;57:1153-62. [Crossref] [PubMed]
- Swaroop S, Arora U, Biswas S, et al. Therapeutic plasma-exchange improves short-term, but not long-term, outcomes in patients with acute-on-chronic liver failure: A propensity score-matched analysis. J Clin Apher 2023;38:376-89. [Crossref] [PubMed]
- Verma N, Choudhury A, Singh V, et al. APASL-ACLF Research Consortium-Artificial Intelligence (AARC-AI) model precisely predicts outcomes in acute-on-chronic liver failure patients. Liver Int 2023;43:442-51. [Crossref] [PubMed]
Reference: https://apm.amegroups.org/article/view/148099/html